Moda Behavioral Health Incentive Program (BHIP): Bold and Reckless?
A Discussion Paper
AMHA (now IMHPA) has been collaborating with Moda Health since 2015. In 2018 the Independent Mental Health Practices Alliance was capable of measurement and value-based contracting . In December 2022, IMHPA began collaborating with MODA for a measurement-based care (MBC) contract and ultimately seeking a value-based payment contract at the end of 3 years.
Detailed documentation, written recommendations and references had been and were provided to MODA based on Federal, State, industry and thought leader guidance. The recommendations included the necessary CPT codes, technology, administrative requirements, progress and outcome measures, data sharing and analysis, and initial communication requirements. The estimated cost for MBC was provided to MODA.
Mentor Research Institute (MRI) believes provider practices involved in the MODA Behavioral Health Incentive Program (BHIP) are being led by MODA into a version of value-based contracting that involves a great deal of risk and very little benefit for them. Further, MRI believes, that MODA has designed their BHIP contract to offer MODA little risk and a great deal of benefit.
What follows is a brief list of questions about which providers need information, education and discussion in order to avoid practicing under agreements that will be to their great disadvantage:

Figure 1. The essential conversation that is necessary to discuss before signing a measurement and value-based payment contract, especially if their is a risk share.
What are fee-for-service, alternative payment, and value-based payment contracts?
What is the future of fee-for-services reimbursements in Oregon?
How do payers and providers get from Fee-for-service to Value-based payments?
What can Go Wrong when participating in a value-based payment contract for psychotherapy (also called “mental and behavioral health services”)?
How do providers Negotiate a value-based payment contract for psychotherapy services?
What are “good faith” and “fair dealing” when contracting for psychotherapy services?
What is a Contract of Adhesion?
How are measurable outcome Base-lines and Benchmarks for psychotherapy services determined?
What are Risk-Share and Risk-Adjustments in value-based payment for psychotherapy services?
What are the Problems that Contracting parties face when creating or entering value-based contracts for psychotherapy services?
Value-Based Payment Contracting for Psychotherapy Services: What Federal and State Regulations apply to such contracting in Oregon?
How can psychotherapists Ensure They Meet the Performance Metrics required by a value-based payment contract?
What are the most important Contract Negotiation Strategies?
What are the most important Strategies to Negotiate value-based payment contracts for psychotherapy services?
What is the importance of Leverage in contract negotiation?
During a conversation with the Moda contract liaison, the MODA liaison presenting the contract had little understanding of measurement and value-based contract terminology and definitions. Subsequent evaluation revealed the contract was probably to almost almost certainly faulty, misleading, ill-defined, and deceptive. During contract negotiation, MODA misled and deceiving the contract negotiator and IMHPA several times. MRI was told by a MODA contract liaison that as many as 128 group practice in several states signed the MODA contract. MODA employees told MRI and IMHPA representatives that they asked questions that no other group practice asked.
MRI came to the following conclusions after collaboration efforts with MODA since 2015.

Figure 2. A Bubble map based on a risk-impacting objectives and risk-control matric.
IMHPA concludes that provider practices were not engaged in good faith and transparent conversation with MODA that otherwise could have resulted in other providers declining to sign their contract.
IMHPA and MRI worked with an auditor to help MRIevaluate the contract. A “risk-impacting objectives” (RIO) and a “risk control matrix” (RCM) analysis was used. The auditor did not offer an opinion but did educate MRI. Based on this analysis, unless something changed, MRI concluded the MODA contract has a probable to almost certain risk of severe to catastrophic impact on public health and provider practices.
The MODA contract has no significant value to over the relative to the downside risk to provider practices and the public. The MODA contract was deemed experiment with no guardrails such as shared values, objectives, controls, and key indicators of success. There is a high financial and moral risk of injury to providers if they participate in the MODA contract as is.
Mentor Research identified 281 requirements and challenges that provider practices must understand if they wish to support or participate in value-based treatment. These requirement could be viewed as opportunities if Moda adopted a collaborative approach.
The MODA contract negotiation systematically turns a blind eye to the requirements and challenges of value-based payments (VBP) (e.g., shared values, objective, controls, test scripts, and leading performance indicators). The contract is best defined as a contract of adhesion (i.e., take it or leave it). MODA is currently unwilling to discuss 281 issues that are important to public health, or to amend their contract language to reflect good faith and fair dealing. forty two of these are critical. By ignoring these issues, MODA retains control and power over provider practices which have no choice but to comply or walk away from the contract. Walking away would mean they will need to accept failure, the financial loss, and loss of credibility with their clinicians.
The MODA contract is a value-based payment contract that has insignificant value to provider practices. The “incentive” is trivial compared to the investment of resources. Rather than invest in provider practices, MODA seems to be assuming governance and administrative control of the contract. The power difference between MODA and Providers is disparate and obvious.

Figure 3. An example illustrating the risk benefit of contract with MODA over the next 3 years.
The MODA contract is a risk-share for which an incentive will be paid to providers if MODA limits the growth in their expenditures on Healthcare services to no more that 5%. It was learned by repeatedly inquiry that Provider practices have no influence over MODA’s expenditures. There are no risk-adjustment provisions for subpopulations because there is benefit to MODA by conflating routine care with urgent care and care for serious and persistent mental and behavioral health problems.
The MODA policy regarding the contract is to deny contact with other provider practices with whom they would be sharing the risk. A risk-share contract required collaboration in order to share information, concerns and to develop common strategies and targets. This created the appearance of measurement and valued based contracting, which would be false because the functional elements for decision making based on an accurate risk assessment was absent.
The State of Oregon has passed legislation to create a research pressure on Healthplans to move from fee-for-service to value-based payment starting in 2021. The State also has proposed legislation that would initiate a research initiative which could create a value-based program that can be adopted by private practice groups. MRI questions CCO values and objectives. Only one CCO in Oregon is a non-profit. Fifteen other CCOs are not.
The MODA BHIP contract is not aligned with important Federal, State, Industry or thought leader guidance. MODA behavior thus far has turned a blind eye to that guidance and IMHPA efforts to bring this to the attention. Provider practices which sign the behavioral health incentive contract have agreed to incentives which have probable to almost certain risk of failure.
MODA has avoided and refused to have the conversations necessary to establish shared values, objectives, controls, tests scripts, or key leading indicators, standard business practices necessary to support success for provider practices and Healthplans. Those standard operational supports are well established in healthcare business operations.
MODA’s BHIP contracting behavior is an example of why value-based payment contracts for behavioral and mental health services have not been successfully implemented in Oregon or nationally.
Discussion Slides Used During Contract Negotiation with MODA.

Figure 4. The steps necessary to create a measurement and value-based payment contract according to the Oregon Health Authority based on and the Centers for Medicare and Medicaid Payment System Learning Action Network (LAN).
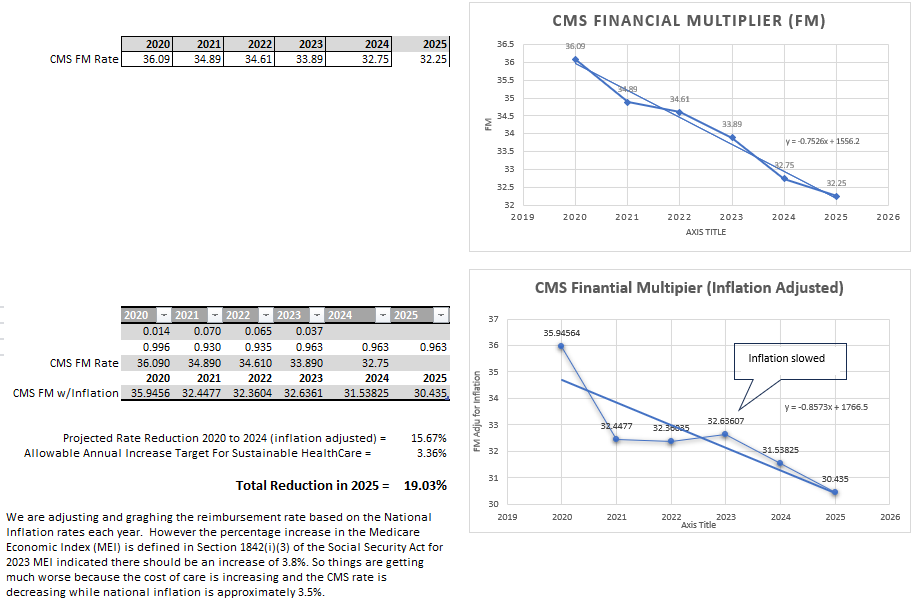
Figure 6. MODA Health’s Reimbursement algorithm changes when 2022 projected to 2025 which provider were not provided; potential evidence of bad faith.

Figure 5. MODA Health’s Reimbursement offers before during and after contracts were signed; evidence of bad faith and unfair dealing.
DISCLAIMER and PURPOSE: This discussion document is intended for training, educational, and or research purposes only. The information contained herein is based on the data and perspectives available at the time of writing. It is subject to revision as new information and viewpoints emerge.
For more information see: https://www.mentorresearch.org/disclaimer-and-purpose